
Health for All Action Plan
2023 Health for All Action Plan
An outline of our process
NOTE: This plan is a work in progress! Since July 2022, we have been working with our community to co-create a new vision for health in the Dan River Region and a plan of action to help us get there. As we continue to engage more residents and organizations in this process, we will continue to update this plan to reflect their contributions.
Download a copy of the one-page plan summary shared during our January 2023 Health Summit.
With a new Health Equity Report, a growing and increasingly diverse coalition, and a much greater understanding of the many factors that influence health and wellbeing, we knew that it was time to revisit our original Health for All Action Plan and to update the approach and strategies in order to better reflect the current needs of the Collaborative and our communities.
Building This Plan
The approach and strategies outlined in this plan are the result of an extensive research and community engagement process including hundreds of residents.
- 2021 Health Equity Report development (23 interviews, 7 focus groups with 43 participants, 697 survey responses, 144 maps and 41 tables)
- Community Conversations (12 meetings, 142 participants)
- Community Ambassadors (165.5 hours of outreach and engagement)
- 2 Regional meetings, 5 Chapter meetings
Key Issues
As we explored and discussed the data and stories from the Health Equity Report, here’s what you told us was most important…
- Access to quality care (cultural competency, LGBTQ+ care, maternal health, mental health, substance use disorder treatment)
- Wealth building and economic equity (education and job training, quality employment)
- Housing access, quality, and costs
- Transportation
- Food systems
- Access to recreation and youth opportunities
- Environmental quality and justice
- Resource awareness
- Leadership development
- Residents as decision-makers, authentic community engagement
- Government accountability
- Community advocacy
- Opportunities to connect, bring people together, and build relationships
- Mindset shifts
Our Big Goal: Everyone in the Dan River Region has everything they need to thrive where they live.
Our approach
The Health Collaborative does not operate programs, allocate resources, or do direct service, but we can make progress in addressing key issues by…
Learning together, activating leaders, and building capacity.
We do this by:
- Helping organizations, institutions, and local governments embrace and implement policy, systems, and environment change strategies that align with our shared values and goals
- Helping individuals advocate for themselves and their communities
- Creating opportunities for both groups to come together to collaborate towards health for all people in the Dan River Region.
Historically, The Health Collaborative has identified focus areas in which chapters and action teams would prioritize their efforts. Though we have made progress in developing and implementing strategies at the policy, systems, and environment (PSE) level, we now have a better understanding of the ways in which all of these strategies intersect and work together to influence our health and wellbeing. We now know that to create the greatest impact, we need to view our PSE strategies collectively, rather than individually, so that they are aligned in ways that move us closer to our shared goal and visions.
As we reinforce our capacity building approach, we recognize that these strategies don’t always fit neatly into any one focus area. Instead, they build up the community’s knowledge and power to be able to address multiple issues at once, thus creating a greater and more sustainable impact.
The descriptions below demonstrate the evolution of our thinking – from narrowly defined focus areas to a comprehensive vision of all the necessary pieces of a healthy community.
Our vision for a healthy Dan River Region includes…
 Active Living: We envision a region where everyone has access to opportunities to be active – physically, civically, and spiritually. Where people are proactive in efforts to improve their health and their community and both physical and social infrastructure make it easy to participate.
Active Living: We envision a region where everyone has access to opportunities to be active – physically, civically, and spiritually. Where people are proactive in efforts to improve their health and their community and both physical and social infrastructure make it easy to participate.

Food Justice: We envision a region with a robust local food system that connects people to healthy, culturally appropriate foods; that provides readily accessible and affordable, nutritious meals for all; and that creates high quality, local jobs across every sector of the food system.
 Access to Quality Care: We envision a region where everyone has access to high quality, affordable care to both treat and prevent illness and harm, and where additional social supports are provided for those with greater needs. We envision a health system that reflects the diversity of our communities, engages in continuous learning and improvement, advocates for improvement of social determinants, and is responsive to community needs both in and outside of the clinical setting.
Access to Quality Care: We envision a region where everyone has access to high quality, affordable care to both treat and prevent illness and harm, and where additional social supports are provided for those with greater needs. We envision a health system that reflects the diversity of our communities, engages in continuous learning and improvement, advocates for improvement of social determinants, and is responsive to community needs both in and outside of the clinical setting.
 Healthy Spaces: We envision a region where all of our homes, workplaces, and shared community spaces are safe, free from environmental harms and hazards, inclusive of diverse populations, and free of barriers to healthy opportunities. We envision a region with enough healthy spaces to support everyone’s health and wellbeing.
Healthy Spaces: We envision a region where all of our homes, workplaces, and shared community spaces are safe, free from environmental harms and hazards, inclusive of diverse populations, and free of barriers to healthy opportunities. We envision a region with enough healthy spaces to support everyone’s health and wellbeing.
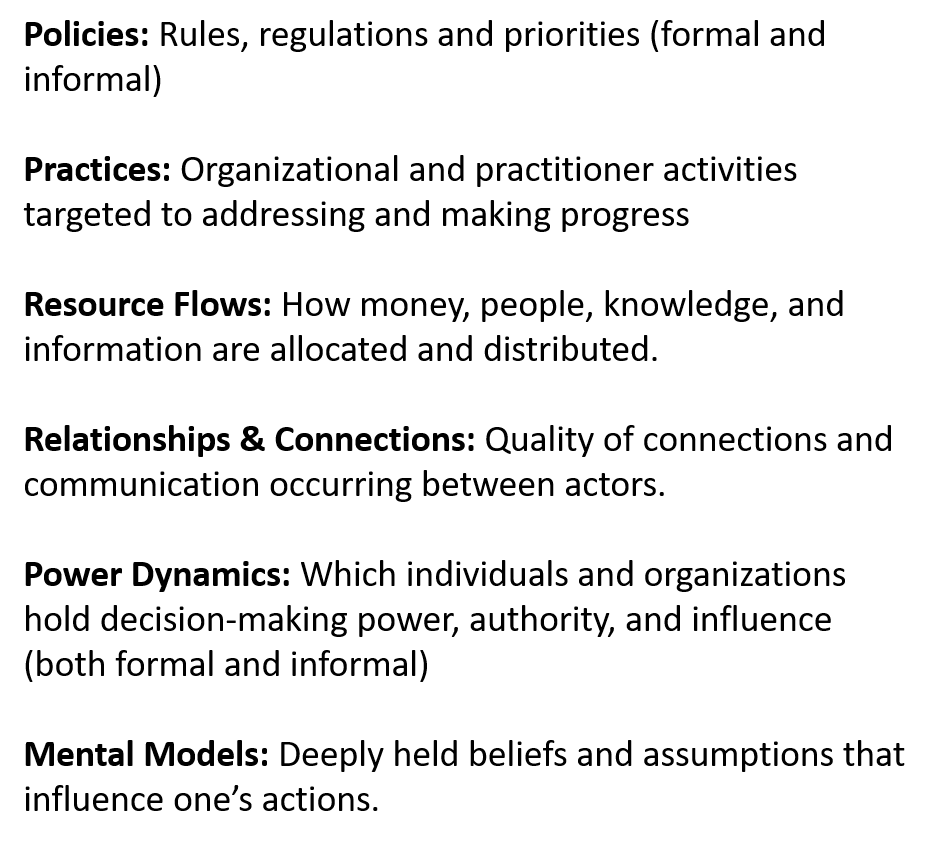
Bringing about this vision for our region is going to take more than just programmatic improvements. It will require systems change. In the “Water of Systems Change Action Learning Exercise”, FSG outlines the six conditions of systems change and asks participants to assess current conditions and identify opportunities to intervene and advance change at the systems level.
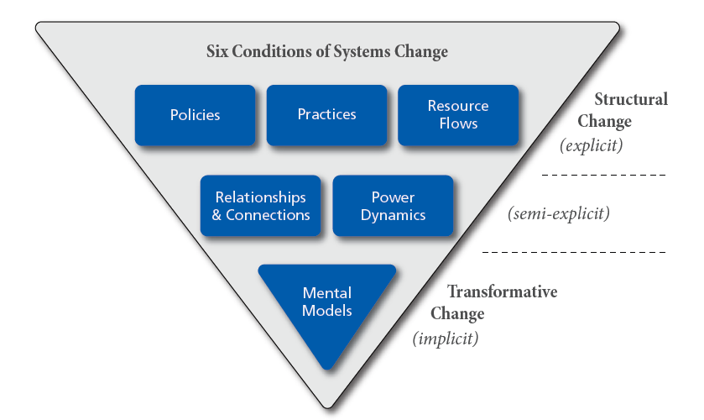
Members of the Regional Health Collaborative participated in the activity and identified the following barriers and opportunities for change.
Active Living |
|||
| We envision a region where everyone has access to opportunities to be active – physically, civically, and spiritually. Where people are proactive in efforts to improve their health and their community and both physical and social infrastructure make it easy to participate. | |||
| SYSTEMS CHANGE CONDITION | What elements are reinforcing the current conditions and hindering our progress? | What strategies can help advance our systems change efforts? Who would need to be involved? | How do we build the capacity needed to do this? |
| Policies | Resident advisory groups with formal decision-making power; policy decisions made based on shared vision for community | Relationship and trust building; shared learning; creating space for residents and decision-makers to connect and collaborate; authentic community engagement | |
| Practices | Planning and building focused on vehicles rather than people; disconnect between residential areas, jobs, green spaces, amenities – creates car dependency; poor communication keeps people unaware of resources or opportunities to participate in planning/decision-making | Collaboration/partnerships with and within government; need more bike/ped infrastructure; transportation infrastructure that connects all essential services and community amenities; improved communication and info-sharing processes (211? Unite Us? Community calendar?) | Authentic community engagement; cross-sector collaboration; federal, state, and local advocacy for more active transportation infrastructure |
| Resource Flows | Transportation infrastructure funds usually go to one govt agency and doesn’t promote collaboration, this leads to car-centric development without consideration for health/equity | Grants, funding streams require cross-sector collaboration | Federal, state, and local advocacy; cross-sector collaboration; relationship and trust building – aligning efforts for collective impact rather than competition; shared learning – Health in All Policies |
| Relationships & Connections | Disconnect between residents and decisionmakers | Park Council, resident park groups | Shared learning; authentic community engagement; relationship and trust-building; opportunities to connect and collaborate; mobilization of residents |
| Power Dynamics | Residents often excluded from decision-making/policy making; same people in office for many years | Resident advisory groups with formal decision-making power; support needed to help others step into leadership roles/run for office | Shared learning; authentic community engagement; relationship and trust-building; opportunities to connect and collaborate; mobilization of residents; leadership development |
| Mental Models | Cars required to get around; decision-makers have total control, need to wait for them to create change; traditional leaders know best; “that’s just the way things are and have always been” | Short trips can be made using alternate/active transportation; residents have collective power and can work together to create change; residents have valuable knowledge and experience to contribute and leaders should value their input; change is possible and necessary | Leadership development; community organizing; relationship and trust building; opportunities to connect and collaborate; authentic community engagement; safe spaces to share concerns and ideas; successful policy change and infrastructure development that will lead to a shift in behavior and mindsets |
Food Justice |
|||
| We envision a region with a robust local food system that connects people to healthy, culturally appropriate foods; that provides readily accessible and affordable, nutritious meals for all; and that creates high quality, local jobs across every sector of the food system. | |||
| SYSTEMS CHANGE CONDITION | What elements are reinforcing the current conditions and hindering our progress? | What strategies can help advance our systems change efforts? Who would need to be involved? | How do we build the capacity needed to do this? |
| Policies | Farm Bill; land use/zoning as a barrier to urban agriculture; policy barriers to mobile food markets; legacy of redlining and segregation has created food deserts | Education around farm bill – what’s included, how does it impact us locally; Local urban ag code updates; policy audit – evaluate all policies related to food systems and amend or remove those that create unnecessary barriers; local food policy council?; alternative food business models – co-ops? | Local, state, federal level advocacy; zoning changes; shared learning; cross-sector collaboration and mobilization for policy change |
| Practices | Limitations of farmers markets; charitable food donations mostly include unhealthy foods | Agribusiness program at PCC creating opportunities for food and jobs to stay local; CEAD project creating new opportunities for beginning farmers (incubator plots), produce sales, education; mobile markets; healthy pantry programs | State and local advocacy for funding that supports projects like CEAD and ongoing food system development; cross-sector collaboration between farms, retailers, schools, businesses, etc. |
| Resource Flows | Food pantries can’t fully meet the need, low wage jobs keep people economically/food insecure; corporate chains make a lot of money in rural communities, but don’t reinvest those profits back into the community | Residents feel confident requesting donations and sponsorships for community events/programming; holding people/businesses accountable to reinvesting in the community; improve job quality | Building relationships between residents, local organizations, and businesses – aligning resources towards shared goals; advocacy at local, state, and federal levels for higher wages and benefits |
| Relationships & Connections | Poor collaboration between schools and farms makes it hard to work together to provide healthy, local food for school lunches | Greater collaboration between farmers, policy makers, and educators – improved farm to school programs/policies | Federal, state, and local level advocacy; shared learning; cross-sector collaboration |
| Power Dynamics | Big agriculture industry pushing small farms out, dominating the political sphere and influencing allocation of resources; food retail corporations merging, monopolizing the market, and raising prices while reducing quality for consumers | Cooperatives and unions for farmers and farmworkers to grow their collective power; a seat at the table for small farmers during policy conversations | State and federal level advocacy, community organizing, building relationships – all sectors of the food system |
| Mental Models | Pride makes it hard to accept help; focus on identity as tobacco region is keeping farmers from transitioning to food production; belief that not going for a 4-year college degree is a deficiency and that farming is a lesser career; eat to be full vs. eat to be nourished; food distribution as charity | Shared prosperity/collective good; farming is a necessary and noble profession – we need good local food!, food security à nutrition security; access to food is a human right | Shared learning, relationship building, cross-sector collaboration, policy change to change mindsets |
Access to Quality Care |
|||
| We envision a region where everyone has access to high quality, affordable care to both treat and prevent illness and harm, and where additional social supports are provided for those with greater needs. We envision a health system that reflects the diversity of our communities, engages in continuous learning and improvement, advocates for improvement of social determinants, and is responsive to community needs both in and outside of the clinical setting. | |||
| SYSTEMS CHANGE CONDITION | What elements are reinforcing the current conditions and hindering our progress? | What strategies can help advance our systems change efforts? Who would need to be involved? | How do we build the capacity needed to do this? |
| Policies | HIPPA regulations related to travel; insurance reimbursement; no more standards of care models – create lack of transparency for patients and places burden on them to research and advocate for themselves; organizational payment plans that restrict access to care for nonpayment | Healthcare reform, better supports for providers and patients, reduce power of insurance companies, reduce influence of corporate money in policy-making | State and federal level advocacy; shared learning cross-sector collaboration |
| Practices | Different perception and treatment of those with private insurance vs. Medicaid; unable to use shuttle across state lines; usable practices; education and workforce development efforts not doing enough to keep people local; lack of cultural competency | Paramedics (those with scope to provide gap-closing care); home health (opportunities); workforce development – healthcare pipeline, incentives to stay local or come to our area; ongoing diversity and cultural competency training | State and federal level advocacy; advocacy for policy change at organizational level; access to continuous learning opportunities; cross-sector collaboration; regional relationship building – across state lines |
| Resource Flows | Lack of transportation support in rural areas; insurance + paperwork; lack of providers; lack of knowledge of available resources; hospitals and clinics not fully staffed; health insurance tied to employment; poverty and lack of household resources needed to practice prevention or appropriately treat illness | Mobile unit; access to local/federal grants; funding and incentives needed to recruit and retain diverse providers; universal healthcare | Cross-sector collaboration – connecting healthcare sector with transportation, housing, food system, education/workforce; shared learning; state and federal level advocacy |
| Relationships & Connections | Disjointed care coordination; distrust of medical professionals/healthcare system; insurance and paperwork requirements add stress to provider/patient relationship; lack of health literacy skills leads to miscommunication | Pipelines with the education system; integrate medical records across various providers; implement trauma-informed practices and health literacy within clinics/healthcare settings | Cross-sector collaboration and alignment of organizational policies and practices (REACH Partnership as an example); state and federal level advocacy; continuous learning opportunities; space for relationship and trust building within our community (bringing patients and providers together) |
| Power Dynamics | Lack of standards of care models affects the power of patients to choose the provider best for them; minority and LGBTQ+ patients don’t always feel that their concerns are being heard or that they have the power to speak up for themselves in healthcare systems lacking diversity; insurance & pharmaceutical companies have too much control over access to and quality of care and use money to influence votes and legislation; people who are sick or caring for a sick person are most vulnerable and less likely to fight the system | County organizations; hospitals and health facilities; reducing power and influence of insurance companies | State and federal level advocacy, access to continuous learning opportunities, space for relationship and trust building within our community (bringing patients and providers together); community organizing |
| Mental Models | Equality vs. equity; not everyone is getting the same level of respectable care; “If I don’t go to the doctor, I’m not sick”; healthcare is about profits; provider assumptions that some people don’t care about their health; denial of the impact of social determinants; belief that health is completely one’s individual responsibility | Move at the speed of trust; safety to voice opinions; need to acknowledge and address personal biases; healthcare is a human right; community conditions have a huge impact on health behaviors and health outcomes; community care vs. individualism | Continuous learning opportunities; space for community dialogue and cross-sector collaboration; local, state, and federal level advocacy; dissemination of data to change thinking; policy change to change mindsets |
Healthy Spaces |
|||
| We envision a region where all of our homes, workplaces, and shared community spaces are safe, free from environmental harms and hazards, inclusive of diverse populations, and free of barriers to healthy opportunities. We envision a region with enough healthy spaces to support everyone’s health and wellbeing. | |||
| SYSTEMS CHANGE CONDITION | What elements are reinforcing the current conditions and hindering our progress? | What strategies can help advance our systems change efforts? Who would need to be involved? | How do we build the capacity needed to do this? |
| Policies | Housing: No competition for utilities; no protections for Section 8 vouchers holders leaves many without access to housing; Environment: pollution, lack of support from local govt | Regulated Airbnb/similar-type places, zoning changes for multifamily housing construction, control over costs; education and policy change to prevent property owners from discriminating against Sec. 8 voucher holders;;Accountability for polluters, need support from BOS, state representatives, DEQ, EPA | Federal, state and local level advocacy; community organizing – tenant organizing?; shared learning; relationships building; cross-sector collaboration – why is this issue relevant to ALL of us?; collection and dissemination of data; building connections with state and federal agencies (DEQ, EPA) |
| Practices | Housing converted to Airbnb, rising costs (rents, etc.) regionally and nationwide; Section 8 discrimination – people have funds needed to rent, but landlords won’t rent to them; Policies in place, but not enforced, polluting industries privately owned, not supporting resident safety | Building multi-unit housing to increase housing stock; subsidy programs; education for landlords on purpose and importance of Section 8 program; Enforce the policies already in place, enforce rules/laws | Federal, state, and local advocacy; community organizing to build power, challenge systems, and create accountability; shared learning; cross-sector collaboration – why is this issue relevant to ALL of us? |
| Resource Flows | Need for better jobs, higher incomes, childcare support; funding lacking; limited capacity for improving housing quality, contractors, home improvement companies working in larger areas; Not enough resources for water/air testing, scientific support | Transitional housing increase (shelters, rescue-mission, etc.), resource hubs, access to financing for ownership; support construction courses/degree at local community colleges; local grants, donations | Collect and disseminate data to demonstrate connections between housing, health, and economy; cross-sector collaboration for comprehensive solutions; federal, state, and local advocacy; community organizing for better jobs, safer housing, safer environment; collect and disseminate data to demonstrate scope of environmental impacts; build relationships and trust with academic/scientific institutions for ongoing research and advocacy |
| Relationships & Connections | Community-wide support is lacking, residents want to see results, but unwilling/unable to put out effort to make it happen; rural social isolation makes it harder to access healthy spaces/opportunities | Need more community support and awareness of the issue | Shared learning, relationship building, community organizing, development of shared vision and alignment of efforts toward that vision; leadership development |
| Power Dynamics | Landlords prioritize “market rate”; Road block with people in power, lack of community-wide support/awareness for the issue, individuals with lots of money and influence control the process; local government not taking resident concerns seriously | Residents empowered, offered ownership opportunities; Need landfill owner to take responsibility for deterioration of community, not continue to proclaim innocence | Shared learning around housing market and government’s role; federal, state, and local advocacy; community organizing and mobilization; leadership development |
| Mental Models | Housing is market-driven, based on making money; Acknowledge that this community is underserved and at a disadvantage | Housing as a human right, not a commodity; Community residents need to change their status from victim to victor | Shared learning; advocacy and policy change to change mindsets; leadership development; community organizing; relationship building |
From there, we identified capacity building strategies needed to be able to enact these changes. We see capacity building as both the essential first step and the continuous process needed to be able to create change at the systems level.
Shared Learning and Leadership
Incorporating learning into all of our meetings; offering training and workshops based on the needs of our community and partner organizations; leadership development; creating leadership opportunities within the structure of THC and providing support for people who want to pursue other positions of leadership; community advocates; using an equity lens; collaborative leadership development
Relationship and Trust Building
Creating space for residents to get to know each other, and space for residents and decisionmakers to connect; offering safe spaces to share concerns and ideas with one another; offering space to process news and events; creating opportunities for productive community dialogue; building relationships across the region, across urban and rural divides, and across state lines; building connections with state and federal agencies; building relationships and trust with academic/scientific institutions for ongoing research and advocacy; supporting the development of systems of accountability and protection i.e. Human Relations Commission
Authentic Community Engagement
Developing and piloting models for authentic engagement; lifting up community ambassador model; supporting the development of resident advisory groups; participatory evaluation; asset-based community development and asset mapping; clear, consistent, and transparent communications – especially between residents, organizations, institutions
Cross-Sector Collaboration
Health in All Policies approach; data collection and dissemination; policy agenda development; asset-based community development; collaborative ecosystem mapping; creating spaces for residents and decisionmakers to connect and collaborate; models for evaluation – measuring commitment to values, coalition effectiveness, civic capacity; communications strategy that is clear and aligned
Policy Change and Advocacy
Shared learning – translation of policy to everyday life; policy tracking at local, state, and federal levels; building relationships with decisionmakers; organizational policy audits – THRIVE!; Health in All Policies; mobilization of residents, community organizing; coordination with state and local advocacy organizations; cross-sector relationship building; development of policy agendas and policy councils; power mapping – who has authority to create change
Over the next several months, the Coordinating Committee and each Chapter will develop its own work plan to prioritize the strategies most meaningful to them and to outline action steps for operationalizing/implementing the strategies.
Thank you to everyone who has been part of this process so far! If you'd like to get involved, reach out to us at info@thehealthcollab.com